One of the more commonsense approaches to reviewing COVID-19 data, amid the outbreak of the ‘Delta variant’, is to look at the percentage of vaccinated people in a regional population, and then look at the percentage of vaccinated people in the hospital with “covid related” symptoms. [Obviously, the presumption is – if the COVID illness is severe enough to require hospitalization, then the patient is severely or acutely sick.]
A review of Los Angeles and San Francisco, California, area populations/hospitalizations previously showed the percentage of hospitalized COVID patients with the vaccine is identical to the percentage of people vaccinated in the population served by the hospital. The same data was reflected in the statistics released by Public Health Scotland (link). The percentage of vaccinated people hospitalized is identical to the percentage of people vaccinated in the population.
♦ What does that mean?
Quite simply, it means the vaccine provides no benefit with a COVID-19 illness severe enough to require hospitalization. So, if the vaccine provides no benefit then why take it, that’s the bottom line question. Before going deeper, first watch this video segment:
https://youtu.be/HuMbRBTZhCY
.
Since that video and discussion above took place in May 2020, we now have a massive number of people who have been vaccinated. Additionally, and perhaps more importantly, we also now have the data on those vaccinated people coming into contact with the COVID-19 virus after their vaccination (‘Delta Variant’). The data is very troubling, because it confirms what was presented in that video.
A review of a sizable data-set from Public Health Scotland shows that 87% of the deaths directly attributed to COVID-19 are amid the vaccinated population [SEE DATA].
 Putting both sets of empirical data together, this is what you discover:
Putting both sets of empirical data together, this is what you discover:
(1) The vaccination provides no benefit to stop the COVID-19 virus infection rate.
(2) The vaccine does not stop hospitalization from severe symptomatic illness.
(2) The vaccine does not stop severe acute respiratory failure that results from SARS-CoV-2 infection.
(3) The vaccinated population that are hospitalized and then die from COVID-19 represent 87% of all deaths.
These troubling outcomes also are confirmed by the Red Cross earlier saying: “Vaccinated people cannot contribute convalescent blood plasma to help other COVID-19 patients in hospitals. That plasma is made up of antibodies from people who have recovered from the virus, but the vaccine wipes out those antibodies; making the convalescent plasma ineffective in treating other COVID-19 patients.”
So, the second alarming question is: Does the vaccine actually create a pathway, an “antibody immune enhancement” that makes the infection more deadly?
Unfortunately, the data starting to come out now seems to say, yes. People appear to have a more severe illness when exposed to the virus after vaccination. That would explain why there is such a high percentage of deaths amid the vaccinated population after exposure.
NOTE: the mortality rate could be a matter of scale. The elderly population have a higher vaccination rate, and the elderly population have a higher hospitalization rate; ergo the older population group, a more vulnerable population group, would make up a higher percentage of people who have died from COVID related illnesses. More study seems to be urgently needed.
Overall, the COVID-19 mortality rate is lower than the flu mortality rate; and both are influenced heavily by pneumonia as the symptomatic cause of death.
♦ Ryan Christian is a researcher who has done a very deep dive into the historic CDC and WHO record of flu cases and now COVID cases. He has an extensive video presentation with dozens of citations from his data research [Main Article].
Christian’s ongoing research indicates the COVID-19 virus is no more deadly than the flu; and Christian uses a historic reference of flu deaths being over-reported and conflated. Citing a hidden 2011 report to the World Health Organization about avian H5N1 and a new A(H1N1) human influenza virus:
WHO (2011) – […] The pandemic policy was never informed by evidence, but by fear of worst-case scenarios. […] In both pandemics of fear, the exaggerated claims of a severe public health threat stemmed primarily from disease advocacy by influenza experts. In the highly competitive market of health governance, the struggle for attention, budgets and grants is fierce. (link)
HHS (2017) – US data on influenza deaths are false and misleading. The Centers for Disease Control and Prevention (CDC) acknowledges a difference between flu death and flu associated death yet uses the terms interchangeably. Additionally, there are significant statistical incompatibilities between official estimates and national vital statistics data. Compounding these problems is a marketing of fear—a CDC communications strategy in which medical experts “predict dire outcomes” during flu seasons. (link)
Those cited historic examples set the baseline to see how three different sets of illness are being conflated in 2021 to maintain a COVID-19 pandemic policy based on fear, worst case scenarios and false data.
From the CDC website they tell us that deaths from pneumonia, influenza and COVID (PIC) are all reported as COVID-19 deaths without differentiation:
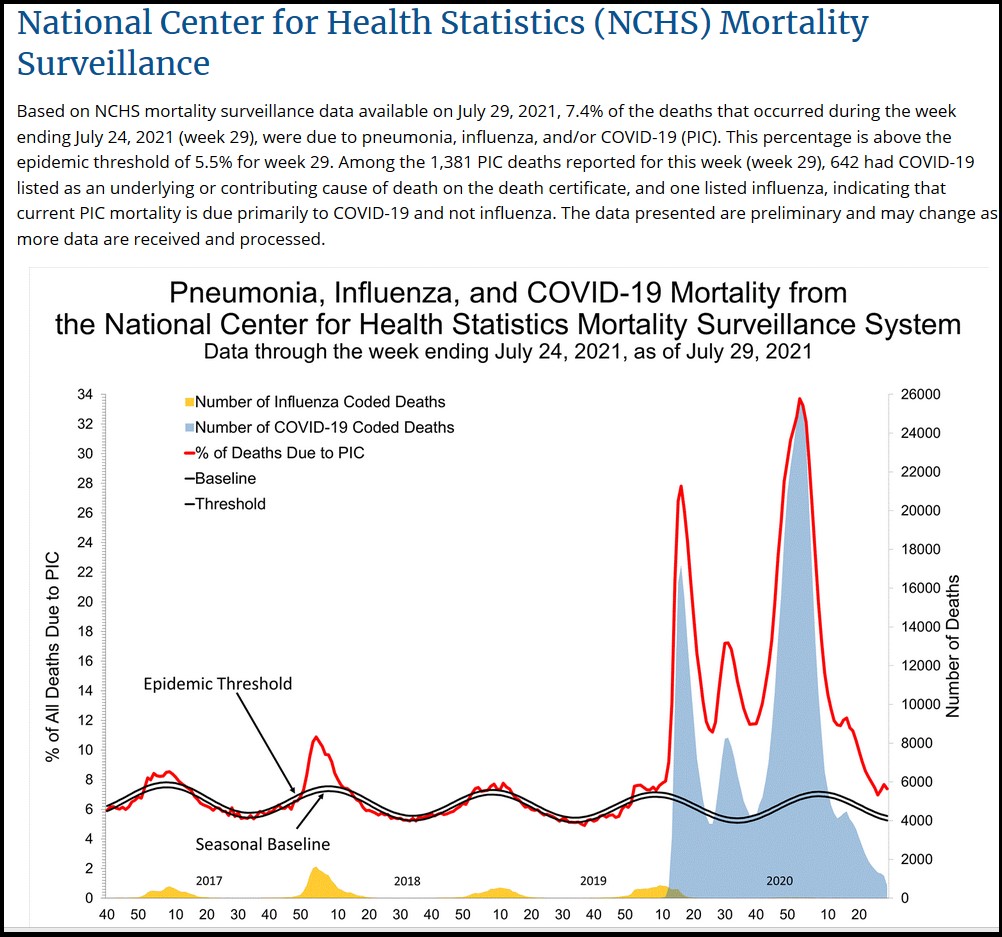
CDC – “Based on NCHS mortality surveillance data available on July 29, 2021, 7.4% of the deaths that occurred during the week ending July 24, 2021 (week 29), were due to pneumonia, influenza, and/or COVID-19 (PIC). This percentage is above the epidemic threshold of 5.5% for week 29.
Among the 1,381 PIC deaths reported for this week (week 29), 642 had COVID-19 listed as an underlying or contributing cause of death on the death certificate, and one listed influenza, indicating that current PIC mortality is due primarily to COVID-19 and not influenza. The data presented are preliminary and may change as more data are received and processed.” (link)
All Pneumonia, Influenza and COVID deaths (the PIC group) are reported exclusively as COVID deaths; and all of that data is dependent on how the hospitals “code” the death. If all deaths are coded as covid deaths, then the CDC mortality data is assembled based on false baselines.
The entire presentation by Ryan Christian is worth reviewing. The discussion is wonky and somewhat in the deep weeds, but everything is massively cited with direct sourcing to back up the hypothesis. [RokFin Video Presentation Here] and his heavily censored Website is HERE.
♦ Bottom Line: COVID-19 is not more deadly than the flu UNLESS you have taken the vaccine; then it might be more dangerous. The vaccine is ineffective at stopping severe COVID illness and, data suggests, might actually make things worse…. creating a perpetual need for continued booster modifications to counteract the initial issue.
There’s something sketchy about the vaccine when contrast against this data, the CDC twisted language, and the scale of government/media pushing and requiring it.
I do not say this lightly.

To jump to the chase, what can we do about the plans for mandatory injections? If we ALL call our congressman will that help? Letters? What?
Since I have heard doctors/scientists – 3 of them – say the being injected will lead to an early death, I am confused, to say the least. that our government officials are so fixated on mandating injections for everyone. Only a conspiracy theory seems to fit the rationale, i.e. population reduction.
Here is 3 hours’ worth of discussion between 3 men who know what they are talking about. Nothing they say about the experimental gene-serum (the “vaccine” that is not a vaccine) is good. Not. One. Thing.
https://rumble.com/viqklz-spike-protein-and-immune-escape-dr-robert-malone-inventor-mrna-vaccines-phd.html
If you haven’t seen this interview of Dr. David Martin, I encourage you to watch or listen to it. It’s a bit long, but he carefully walks through the evidence, using patent records, that the faux pandemic was in the works for decades because there is very big money to be made from manipulating viruses and then producing “vaccines” that cause more illness.
https://odysee.com/@vaccines-covid-nwo:3/JgxEMA02opvp:6?
Great and true article. Hence, why we did NOT take the vaccine. Ask yourself, what happened to the “yearly flu” deaths? This “Vaccine” is via Bill Gates who wants to cull the world population – lots of evidence of that in past years. I live my life “fearless” every day in every way. This “vaccine” is one more way for the Drug Companies and many others to make money! Masking is only about control and Biden/Dems and RINO’s are all invested / in bed with Corporations, especially the drug companies. Fauci has been inept for his 40 plus years at the CDC – he should have been FIRED long ago.
https://healthy-skeptic.com/2021/08/05/the-cdc-also-known-as-the-coronavirus-dunce-collective/
Crispr/cas9
Dr. Fauci in the Wuhan lab with the shears!
Did I win?
peter daszak in the ngo with the grant. please distribute any winnings to tina forte’s campaign.
Makes you dependent on the vaccine. Booster shots forever.
https://pubmed.ncbi.nlm.nih.gov/32908214/
If you follow the common sense and logic, you don’t want or need billions of pathogenic spike proteins circulating in your bloodstream, causing blood clots and vascular disease, not to mention ADE.
ADE is a separate matter brought on by cytokine storms, the immune system’s over-reaction to (otherwise benign) subsequent coronavirus infections.
The “experts” already knew this was a catastrophic sequence. That’s why they insisted that the shots remain in the arm muscle and then quickly dissipate. That was another lie.
I believe that early treatment with blood thinners can prevent the micro clots caused by clumping spikes and prevent them from escalating to heart attacks and strokes, by giving our immune systems time to recover from the initial onslaught of pathogenic spike protein injections.
Maybe our immune systems can eliminate the threat before it causes a severe vascular disease.
The “booster” shots will continually introduce billions more of these spikes, to ensure that our immune systems never have a chance to eliminate them.
Don’t take the booster shots.
Maybe the vaccinated can avert further damage if they treat to allow their immune systems to eliminate that first batch of spike proteins before they cause heart attacks, lung and brain damage and strokes.
If the gene-therapy vaccines worsen the severity of symptoms related to SARS-CoV-2, you can use what PT did.
-8-Gram Dose of COVID-19 Antibody Cocktail Provided to President Trump
REGNCOV2 provided to President Trump under Compassionate Use Request
https://www.precisionvaccinations.com/8-gram-dose-covid-19-antibody-cocktail-provided-president-trump
-FDA authorizes REGEN-COV monoclonal antibody therapy for post-exposure prophylaxis (prevention) for COVID-19
https://www.fda.gov/drugs/drug-safety-and-availability/fda-authorizes-regen-cov-monoclonal-antibody-therapy-post-exposure-prophylaxis-prevention-covid-19
“COVID-19 antibody therapy is authorized;
“in the trial the therapy reduced the risk of COVID-19 development by 81% compared with placebo.”
Aren’t these the antibodies derived from recovered COVID-19 patients? If so, it would follow that your own prior Covid-19 exposure would also afford you the best protection from future infections.
So why did the World Health Organization recently change their website to eliminate this reference to natural immunity? And why do the Vaccinators push unnecessary injections on already recovered COVID-19 patients? They obviously have the best possible immunity already!
“… Covid-19 exposure would also afford you the best protection from future infections.”
That’s what the experts I’m listening to are saying. And even SATS-CoV1 memory would, as well.
now tell me who’s that lying? joe the vaccinator, ’bout the jab that never heals.
I do not believe there can be a “NATURAL HERD IMMUNITY” given the fact that we are dealing with a GENETICALLY ENGINEERED, BIOLOGICAL WEAPON. Indeed, with the 4th VERSION released from SOCIALIST CHINA, there is so little “BAT SPEW” left, as compared to the first 3 released, that the testing kits have to be “RE-CALIBRATED” in order to actually DETECT it accurately.
But then, I am not a “VIRAL WEAPONOLOGIST”.
Although, in my youth, I did spend countless hours “PLAYING DOCTOR”.
DEPLORABLE JEDI.
Three names for same thing I believe
ADE – Antibody Dependent Enhancement
AIE – Antibody Immune Enhancement
Pathogenic Priming
Dr. Roberts Malone – inventor of the mRNA technology behind the vaccines is all over this. Google him before Google, Biden and Fauci make him disappear.
This was when Trump was in office and everyone was OK with anything that would criticize his efforts on anything. Have these concerns now mysteriously disappeared? Not a single mainstream talk show discusses this anymore.
So most vaccinated people are Democrats and 20 to 30% will die due to pathogenic priming.
Works for me.
Unfortunately both my beautiful daughters took the JAB. both are nurses and hated Trump so they kissed Biden & Kamala’s atse. So sad & broken hearted. They also lost all fear of God our Creator.
If, as stated in the video, people are being prosecuted for failing to research the vaccine’s pathogenic priming, WHEN WILL FAUCI BE INVESTIGATED? And TRIED? Two things these tales of vaccine-prompted escalation of infection have in common: Anthony Fauci is peddling them. Bill gates is funding them. (And I’ll bet a dollar that, dig deep enough, Klaus Schwab has a finger in this homicidal stew as well).
Quoted statement from the Red Cross in which it is said the vaccines kill one’s natural antibodies against C19??? I feel “ignorant” as this I swear is the very first time I’ve read anything that calls this out. And just proves the brain wizards running this f-show didn’t give 1 second of thought as how to explain what the vaccines do to those with serious questions.
If true, then WTF is in the vials? “They” say mRNA tech. instructs cells to make 1 spike protein so your body’s immune system kicks-in to build anti-bodies, but if it also kills-off natural C-19 antibodies, then WTF???
None of this makes any sense….
Ever had a pedophile exposed? And looked back at all of that person’s interactions?? In hindsight …
That is the mind we are facing. It has to decieve, lie, and flirt to survive
That part made me sit up too. Are they saying that if a person who had Covid gets a vaccine, their natural immunity will be destroyed?
That is how I read it. Can not believe that was not reported, I know a few people that recovered from covid and got the vaccine anyway.
In July I had covid. One night couldn’t breathe so my son took me to ER close to our home. The young dr and his minion tried to talk me into getting Vaccinated while I’m fighting for my breath and life. After 5.5 hrs of bs tests and still no oxygen I demanded to be released. I’m pretty much over that evil thing except weakness and coughing. I’m 64 and have a stent, other respitory issues. That hospital has all my record yet no one helped me but I made it. Can’t trust anyone related to this cash cow industry.
And I’ll bet no one offered you Ivermectin, steroids, or monoclonal antibodies, right? Nope, it’s vaccine or you’re left to die. And vaccine while you’re infected would do NOTHING for you.
Read Coast’s reply below. It doesn’t make sense because it isn’t true.
Scientifically, I don’t know how vaccine-induced anti-spike-protein antibody formation would suppress the broad-spectrum antibodies generated through Covid infection.
What is interesting is that the Red Cross disqualifies vaccine recipients from donating plasma. If the vaccines’ anti-spike-protein antibodies were protective against Covid infection, one would think that vaccinated-donors’ plasma would be useful to treat Covid infection.
The dual monoclonal antibody prep REGN-COV2 that helped PDJT is comprised of two antibodies that bind the Covid spike protein. https://www.nejm.org/doi/full/10.1056/NEJMoa2035002
This prep is, like the vaccines, not FDA approved, but allowed under an EUA.
What is mind-boggling is that a high-tech anti-spike-protein antibody-formulation is authorized, while plasma containing anti-spike-protein antibodies is disallowed. (The Red Cross doesn’t make up its own rules, it obeys FDA dictates.)
Our son is currently enrolled in PA school, has three years as a Medical Lab Tech, and has a degree in Biology and Medical Laboratory Science. I asked him about his article….here is his response:
Logical flaws all around.
They claimed that San Fran and LA have been seeing equal numbers in hospitalizations from vaccinated and unvaccinated individuals. On the surface, that sounds troubling and as if the vaccine doesn’t work. But then let’s consider proportions. San Francisco has a vaccination rate of around 80% last time I checked. So if San Fran has a fictional population of 100 people, 80 are vaccinated, 20 are not, and in both groups we see 5 people get COVID, then it becomes obvious that the vaccinated group has a very low proportion of positivity (6.25% in this example) while the unvaccinated group has a massive positivity proportion (25% in this example). However, I don’t think their claim that hospitalizations were equal was even accurate as they were citing a chart that was posted by someone on twitter about data from UCSF that I, and others, couldn’t find on UCSF’s website.
This same flaw was used to evaluate the Scotland public health data. They looked only at the number of hospitalization among unvaccinated and vaccinated (note that they incorrectly interpreted the data to say that people who have had a single dose are vaccinated when we know empirically that a single dose does not properly protect from COVID). In Scotland, they too have a very high vaccinated rate; around 70%. Therefore, if the sheer number of hopitalizations are equal among vaccinated and unvaccinated, that still means that the vaccinated have a lower proportion of individuals requiring hospitalization.
Their claim “all Pneumonia, Influenza and COVID deaths (the PIC group) are reported exclusively as COVID deaths,” is just wrong. It’s an exceptionally complicated subject as medical billing can list multiple contributing factors for deaths but the CDC has reports currently on influenza and there is a clear delineation in reporting for these. If this claim was correct, hospitals would be failing inspections as they would be incorrectly billing insurance providers, alerting patient records, etc. It just isn’t happening.
Their bottom line statement “COVID-19 is not more deadly than the flu UNLESS you have taken the vaccine; then it might be more dangerous” is laughably bad and plain fearmongering. It’s patently false and there is so much data out there showing the proportion of vaccinated people requiring hospitalization and eventually dying from COVID is extremely low when compared to the unvaccinated population.
They also falsely quoted the Red Cross. They have an explicit line on their website even to try to combat this lie:
Q: I’ve heard claims that the Red Cross refuses to accept convalescent plasma from individuals who have received a COVID-19 vaccine because it wipes out the antibodies. Is this true?
A: There are claims circulating that incorrectly state that the Red Cross will not accept convalescent plasma donations from those who have received the COVID-19 vaccine because “the vaccine wipes out those antibodies making the convalescent plasma ineffective in treating other COVID-19 patients.” This is not accurate.
The FDA allows people who have received a COVID-19 vaccine to donate dedicated COVID-19 convalescent plasma within six months of their infection of the virus, based on data that antibodies from natural infection can decline after six months.
The Red Cross discontinued dedicated COVID-19 convalescent plasma donations on March 26 due to declining hospital demand and sufficient industry supply. The Red Cross tests all blood donations for COVID-19 antibodies. Plasma from routine blood and platelet donations that test positive for high-levels of antibodies, and meets other requirements, may be used as convalescent plasma to meet potential future needs of COVID-19 patients.
Is that how you protect yourself? You go to the suspect and ask them to tell you what to think
Low iq response.
A brain could see that a virus with less than 1% chance of killing you , being pushed as a 99% chance of killing you MEANS SOMETHING WRONG and DECEPTIVE is going on
And it takes nothing to tell some punk at the red Cross to edit the website cause you are screwing our goal up of pure control
Use the actual admission number and their actual vaccinated statuses so we can speak in Real Land and not Democrat hypotheticals
I’ve never seen a statistic of “99% chance of killing you” being used. Is Covid being over-blown by the media and being used against liberty in certain areas of the country…sure, but trying arguing that with the people who are currently on ventilators or who have died. Properly inform yourself.
Old, sick, helpless people who were put on ventilators with a 20% chance of survival, while people like Fauci knew good and well there were safe, effective treatments available that would have saved a lot of them? And that those treatment were being suppressed to ensure high death numbers among expensive Medicaid patients…yeah, I do like to think about them a lot.
Excellent reply. On this topic, CTH and other similarly aligned information resources have turned into echo chambers pushing a narrative by selectively examining and presenting information to only point in one direction. Unfortunately, it requires considerable time and research to get at the truth. Like your son, I have an informed resource – an immunologist who is a trusted friend. It certainly doesn’t help that CDC, WHO, Big Pharma, Big Tech, and the media are simultaneously peddling the vaccines to the exclusion of therapeudics and without being fully transparent about vaccine risks until it is blindingly obvious (e.g., myocarditis link). But two wrongs don’t make a right…CTH is regrettably doubling down on a narrative that is being advanced using half-truths and distorting data.
what do you specifically say is BULLSHIT that CTH wrote?
You honestly CANNOT go to the redcross website now, and say it doesnt say what CTH said it said. BEcause you know websites can be edited just like this MESSAGE CAN.
see – i edited this message, just then… (what did i change?)
So your saying the vaccine is sterilizing? That it gives immunity or stops the spread? What exactly is your point and why should we be forced to take this experimental gene therapy?
Sorry Blue Hen, don’t buy it. CTH welcomes alternative views and for you to paint a broad brush that CTH is an echo chamber is BS. Sound like cancel culture. There is a big elephant in the room that is totally missed by Sundance and this thread. I am getting my information from other sources than CTH such as medical published papers, links which I have posted previously. Collectively, WE ARE NOT AN ECHO CHAMBER and to state that is false. We are a crowd sourced information research group. Not perfect by a long way, but we are what we are.
Here is what what the elephant is:
ADE. We should not be looking at Vax Covid deaths, we should looking at all death with the Vax. I have seen nothing posted here or by the CDC or anywhere else that talks about that. How many deaths accorded from all cases after 1,3, 6 9 months after the vax.
Whiteboard is on track. Asking the question able admission numbers and reminding us of risk levels. Context is everything.
Medical professional that I have talked to that are concerned about the Vax point to their anecdotal experience that radiology studies show the short term impact of the effects of the Vax including issues with breast tissue on the side of the body where the vax was given. Based on that along, VAERS seems to validate that the Vax impacts other organs in the body. Enough so to be concerned. Enough to validate what the FL and other doctors are saying.
The Vax is going to be massive in comparison to Thalidomide.
https://www.cbsnews.com/news/german-drug-company-apologizes-for-notorious-drug-thalidomide-50-years-later/
I only see a few solutions to this. HQ or Ivernmectin. By stopping the virus before is goes wild will give the Vax the best chance of stopping this. Same for us.
Ryan Cole sums it up pretty good.
https://www.londontimes.live/health/dr-ryan-cole-blows-the-whole-cov-19-propaganda-away/
Same with Malone:
Sorry Blue Hen, but Sundance was actually holding back and trying hard not to be alarmist.
Forget the argument over ADE style Disease Enhancement. You can play all the games you like to suppress the warnings and lead more into the trap.
But there’s one thing you can’t hide: the “fully vaccinated” are both catching and spreading the virus. This means that the “vaccines” are non-sterilizing. And the mass use of non-sterilizing “vaccines” in a pandemic is guaranteed to accelerate viral evolution.
You can thrash, flex and writhe like a weasel on methamphetamine, but there can be no escape. Too many nations have opted to save their citizens before the Davos elite.
There’s no point in fighting on. Remember the rule of holes ..?
So we should be forced to take the “vaccine” in you sons opinion?
Did he say that? No…he didn’t. Should we take the vaccine….generally yes. We personally know several people who have had Covid…and most had a rough time with it…in fact three people that we are close to seem to be suffering with long-term consequences. We also know of people that have died from Covid. Our son’s room mate from last year got Covid, but for him it wasn’t a problem, and our son didn’t catch it.
This manufactured virus seems to be a hit or miss sickness. With my past lung scaring from pneumonia (which I had as a child) is not a good recipe for an illness that attacks the lungs. Do what you want, but people need to be better informed than just listening to a single narrative.
Generally yes? The data is overwhelming, the “vaccine” is not sterilizing and that is a scientific fact. The risk from the vaccine outweighs the risk of the virus. Therefore the need to take it is moot. Any other reasoning is brainwashed psycho babble. You and your over credentialed son, Fauci Jr, have a nice day.
People come here because that single narrative is found everywhere else. If the “vaccine” was truly effective the government wouldn’t need to resort to threats.
^^^This, right here. If the virus was making healthy people drop dead in their tracks, and the vax was stopping that, people would be flooding in to get it. You wouldn’t have to bribe, coerce, and suppress information to make them do it.
Roommate? Are you implying this was a young, healthy person? I’d really love more detail, because those deaths in actuality are rare as hell, like one in a million. Really makes me doubt your “my son is…” story.
Wow. This is complete disinformation. If this is the training ground, no wonder we have so many clueless doctors out there.
Where to begin?
First off, I don’t believe any statistics these agencies spew about “percentages” of anything. We all know how the so-called experts routinely skew their models to obtain a desired outcome.
For example:
In vaccine trials for safety, those who had problems with the first injection and didn’t get the second, were eliminated from the trial. So the quoted statistics stuck only with those who had two injections, and then only for the first fifteen days, and totally ignored any “drop outs” who exhibited side effects from one injection.
Also, all things being equal, nothing is actually equal at all. The CDC admitted that it changed it’s protocols for testing, making it easier to scoop UN-vaccinated people into a “positive” category and not look for same in vaccinated people.
So.. are vaccinated people really not getting COVID, or are they not getting TESTED for Covid? Unlike the UNvaccinated, who are tested every time they turn around sick or not, the vaccinated are tested only when they are hospitalized, and even then the cycle is run low (NOT looking for that proverbial needle in a haystack). The CDC spells this all out right on their website, unless it was scrubbed again.
And that is another problem: CENSORSHIP. Whenever an inconvenient truth escapes to threaten the preferred narrative, the information is magically altered if not scrubbed from the internets entirely. We have highly respected doctors and scientists in the field who can’t get a word in edgewise. This included Nobel prize winners, scientists and even the inventor of the MRNA technology. All their prudent warnings were SILENCED.
Bottom line: If we cannot trust or even question the “hard data” fed to the masses by known propaganda purveyors like CDC, WHO, FDA, Lancet and just about every alphabet agency, it is best to look at the simple, barest facts.
•The injections do NOT provide immunity from coronaviruses.
•The injections do NOT prevent infections from coronaviruses.
•There was no “emergency” pandemic because the survival rate was was well above 99 percent before “vaccines” were introduced.
•The FDA should not have approved *any* emergency use human experiments since there were safe therapies available (but suppressed by Lancet, killer Commo and others).
•Vaccinated people are now hospitalized with serious symptoms. So they are getting very sick for some reason.
•Testing for Covid-19 is arbitrary and does not rule out other viruses. (And yes, the regular 2020 flu statistics either miraculously disappeared or were rolled into the Covid-19 statistics to make them appear much worse).
•UNLIKE Covid-19, which did not affect healthy young people beyond a mild cold, VACCINATED young people are experiencing SERIOUS side effects like blood clots, myocarditis and pericarditis. BAD INJECTIONS!
I have no use for the Red Cross, which was also knee deep in that 2014 Ebola fiasco, with the fake Doctors Without Borders fanning out like cockroaches to spread this highly contagious AND deadly disease with no thought for CONTAINMENT.
Nobody with half a brain wants to introduce EXPERIMENTAL MRNA technology into our blood bank. If they do then they are irresponsible morons.
I’m not going to argue with your comment except to say that your statement below is completely false. If they did that, then it’s not a trial…and they didn’t.
(In vaccine trials for safety, those who had problems with the first injection and didn’t get the second, were eliminated from the trial. So the quoted statistics stuck only with those who had two injections, totally ignoring any “drop outs” who exhibited side effects from one injection.)
I was about to reply with a reference to an article from America’s Frontline Doctors dot org. But when I went to find it, their entire website has been removed (!)
So there ya go.. CENSORSHIP!
Coast, I’m sorry you took the shots instead of the Ivermectin.
Face reality. Disease Enhancement is occurring. Is it Antibody Dependent or cellular pathway? It’s actually not important.
Denying it doesn’t solve anything for you or anyone else that took the shots.
Coast,
It’s great that your son is in PA school. My son is a PA. He doesn’t know as much medicine as his M.D. parents, by a long shot.
I didn’t learn that much about virology and immunology in med school. Fortunately my undergrad double-major in biochemistry and molecular biology in a world-leading research university, which included 2 years laboratory research training under a molecular virologist, who was yooung at the time, but was subsequently elected to both the National Academy of Sciences and the Institute of Medicine, and a year’s worth of graduate courses in molecular biology and immunology, gave me a lot of info that was not taught to medical students and residents. For example, I read several papers written by immunoregulation giant Niels K Jerne (Nobel Prize Physiol or Med 1984). If you read Jerne, you learn that vaccines are far from the “magic bullets” that public health experts proclaim.
On the SF data, I agree with your son’s position.
On the Scottish data, the authors demonstrated that although unvaccinated people’s infection and hospitalization counts were higher than vaccinees’ counts for the entire period of Dec. 2020 through July 8 and July 8 July 15, 2021, for much of this period, very few Scots were vaccinated.
In contrast the death counts for the period July 8-July 15 were 5 unvaccinated vs. 28 fully vaccinated (from about a 1:2 ratio of population unvaccinated vs. vaccinated). The authors did not perform a P-value discrimination test, but fundamentally, if the vaccinees’ constituted 2/3 of the population, their death count should have been roughly twice the death count for the 1/3 unvaccinated. Instead it was nearly 6 times higher.
I was once a biostatistics maven, but have not done biostatistical analyses since the mid-90’s. I can say this: A death count of 1 in group A vs. a death count of 6 in group B is not statistically significant. A death count of 100 vs. 560 is highly significant (P<0.00001). 5 vs. 28 may be significant (P<0.05) to very significant (P<0.01), but I doubt it is insignificant.
Most importantly, if future death counts are accurately reported, we shall find out if this preliminary data bears fruit or not.
Finally, you said,
The Red Cross discontinued dedicated COVID-19 convalescent plasma donations on March 26 due to declining hospital demand and sufficient industry supply. The Red Cross tests all blood donations for COVID-19 antibodies. Plasma from routine blood and platelet donations that test positive for high-levels of antibodies, and meets other requirements, may be used as convalescent plasma to meet potential future needs of COVID-19 patients.
Which is it Coast? These are two mutually-contradictory things. If the RC reopened plasma donations after March 26, you have failed to state this. If your last statement was RC’s policy from before March 26, but is no longer in effect, you’re engaging in sophistry. Which is it?
Regarding the deaths in the two groups ( 5 unvax’d and 28 vax’d) I wonder what % of them were in high risk categories – healthcare workers, elderly, immune compromised, etc.
It seems possible to me there could have been more high risk people in the vax’d group. They may have been more incentivized to take the vaccines.
The article did not state that the hospitalizations in Scotland among the vaccinated and the unvaccinated are equal. It said that “87% of the deaths directly attributed to COVID-19 are amid the vaccinated population.” That is not equal, that is lopsided on the vaxxed.
The are those of us who’ve been saying this for well over 18 months….
French Virologist and Nobel Prize Winner Luc Montagnier says that it is the vaccine — not Covid — that is causing the variants …. Link to short video in article (French with English subtitles)
https://rairfoundation.com/bombshell-nobel-prize-winner-reveals-covid-vaccine-is-creating-variants/
An opinion from a critical thinker to the question posed in the title of this article.
https://rumble.com/vksdg4-the-never-ending-covid-variant-fear-parade.html
How are we who believe this information going to be able to keep from getting this vaccine?
Comment self-redacted, pending another look or three, at my reference…
Is Gavin Newsom really Nanzi P’s nephew?
His father’s sister, Belinda Newsom, married Ron Pelosi in 1956. This made Ron Pelosi Gavin’s uncle-in-law. Did this make Ron’s brother, Paul Pelosi, Gavin’s uncle-in-law once removed? Paul married Nancy. Did this make Nancy Gavin’s aunt-in-double-in-law once removed?
Ron and Belinda had children. So Gavin has Pelosi first cousins by blood through Aunt Belinda. These cousins are also first cousins by blood to Paul and Nancy’s children–but the latter are of no blood relationship to Gavin whatsoever, as they do not have Belinda’s genes.
At any rate, not only is Gavin not of any blood relation whatsoever to either Paul or Nancy, his aunt Belinda divorced Ron Pelosi 44 years ago, so I don’t know if a relationship by marriage long ago dissolved confers “aunthood-newphewhood” today. This is not to say they don’t have “extended family ties” (wink wink).
My kids call my sister’s husband “Uncle Rick”. They do not call his brothers “Uncle”, nor their wives “Aunt”, though their first cousins rightfully do.
“Logic” is often a tough subject to grasp, so it’s good we’re all working on it..
I know a guy in his 40’s that works around Army Soldiers. From Nov 2019 to March 2021, he never contracted the China FLu (Yes, the China Flu has been here in WA State since Nov 2019). In March 2021 he got his 1st Pfzer Jab and 1 week later he ws in the hospital & almost died from the China Flu. He said his Wife also fell sick, she had no jabs & wasn’t hosptializd. Dude still went and got his 2nd jab.
Can’t fix stooopud
“Does the vaccine create a pathway to a more dangerous variants?”
Yes (but maybe no).
Addressing the “yes” part, it is well known that non-sterilizing immunity always has the potential to do that.
https://dryburgh.com/geert-vanden-bossche-mass-vaccination-danger/
Since that is what this immunization is, then that’s what we should expect.
Note – it isn’t a vaccine in the classic sense, which gives blanket long term broad immunity. It’s an immunization against the original spike protein which doesn’t exist anymore, except in a N2l freezer somewhere.
As to why the variants, produced in the inoculated, may not be worse – since the original was optimized for humans, I would expect it can’t get any worse than when it first struck. I could be wrong, but it seems likely to me. BUT, if better, worse or no different in outcome, it’s still the immunized who are unwittingly producing them, not the untreated. (Think of how resistant bacteria arise from overuse of antibiotics. Selective pressure only exist in the inoculated.
For more on the biology, immunology and virology, please visit….
https://m.twitch.tv/videos/1109331513
His informative videos are very helpful in deconstructing the nonsense coming out of the MSM and politicians.
So the vaccine is a death trap we know this and this why all liberal should be exterminated oops I mean vaccinated now I personally know 2 people recently diagnosed with cancer after getting the jab. And 1 I know for sure was getting regular blood tests every 6 months for years now first blood test after his jab well what do you know prostare cancer surprise surprise
https://onlinelibrary.wiley.com/doi/10.1111/ijcp.13795
There is no informed consent.
Laws are no longer for our protection, but are either ignored or have become a club to beat us with.